LA NECESSITA’ DI
CAMBIARE STRATEGIA PREVENTIVA DELLE VARIANTI DEL SARS-COV 2
PER LA PREVENZIONE DEL
COVID-19 E DELLE MALATTIE TRASMISSIBIL
Giuseppe R.Brera[1]
Riassunto
La continua produzione di varianti
del SARS-COV 2 dovuto al cambiamento dello Receptor Binding Motif delle Spike
Proteins causato dalle caratteristiche del virus e dalla vaccinazione di massa
in tempo di epidemia che promuove l’evasione immunitaria del virus, porta a una
ritardo della produzione dei vaccini rispetto alle infezioni e alle sindromi
cliniche, fatto che non può prevenire il diffondersi di nuove infezioni.
Inoltre i vaccini mRNA sono genotossici e causano una grande incidenza di
effetti avversi anche mortali che hanno portato in alcuni stati alla
sospensione di ogni vaccinazione in bambini-adolescenti e giovani sotto i 39
anni.
Le prevenzione del
COVID-19 in Italia è stata affidata dal Dicembre 2021 a una vaccinazione di
massa con sieri vaccinali sperimentali a mRNA e adenovirus vettoriali
provenienti da scimmie e da feti abortiti il cui DNA s’ibrida con alta
probabilità nel DNA del vaccinato, aumentando la probabilità di malattie
autoimmuni e altri problemi anche psico-neurologici. Prima del 2021 e dopo non c’è stata
prevenzione secondaria nella popolazione a rischio, anziani con comorbidità e
persone con patologie aterosclerotiche, malgrado la ricerca sul SARS-COV del
2002-2003, e della MERS 2009-2019, scomparse senza vaccini con l’immunità di
gregge. La prevenzione primaria è stata limitata al lock-down, l’insegnamento a distanza,
l’uso di mascherine facciali e al
lavaggio delle mani (senza indicare la
temperatura virocida) e la loro disinfezione insieme agli oggetti toccati,
omettendo completamente semplici tecnologie disponibili da anni. Una obsoleta prospettiva epistemologica e gravi omissioni nell’organizzazione della
prevenzione hanno portato al “lockdown”, a obblighi vaccinali senza validazione
scientifica delle possibilità di contagio, penalizzando il lavoro e l’economia. L’uso delle
mascherine e l’insegnamento a distanza hanno penalizzato la salute mentale di
bambini e adolescenti e impedito l’instaurarsi dell’immunità di gregge
esponendo i bambini a una maggiore vulnerabilità per altri patogeni. Gli errori
ed omissioni nella prevenzione primaria e l’omissione della prevenzione
secondaria nella popolazione con comorbidità (93% della mortalità), ha causato
in Italia più di centomila morti e nel mondo milioni di morti. Le indicazioni
sbagliate per le cure domiciliari precoci “ Tachipirina e vigile attesa” da parte
del Ministro della salute italiano e lo scarto di terapie efficaci ospedaliere
come i sieri iperimmuni di convalescenti hanno causato migliaia di morti.
Attualmente la rapidità
delle continua produzione di VOC (Variables of Concern) e l’inefficacia delle
vaccinazioni precedenti per il “peccato antigenico originale e
l’immunodepressione causata dai richiami, porta sempre a un ritardo della
produzione di vaccini mRNA efficaci, ma evanescenti e pericolosi per l’induzione
della metilazione cellulare di tutto l’organismo che aumenta la vulnerabilità
ai tumori. La sperimentazione clinica dei vaccini mRNA fatta dalla Pfizer
inoltre è risultata inattendibile, in particolare quella sui bambini. Gli
effetti avversi dovuti al terremoto epigenetico sono frequenti e anche mortali.
E’ urgente un cambiamento della
strategia preventiva primaria e secondaria e un’organizzazione domiciliare di
cure precoci basata sulla Medicina centrata sulla persona, cambiamento di
paradigma della scienza medica, che se praticato, avrebbe bloccato l’epidemia
sul nascere.
La prevenzione primaria estesa a
tutta la popolazione comporta educazione alla salute e alla “sel care” basata sull’allostasi
antivirale e l’immunostimolazione preventiva, secondaria sull’individuazione dei
pazienti a rischio, l’organizzazione delle cure domiciliari precoci con l’indicazione
di efficaci anti-infiammatori-anti virali di sintesi e naturali.
La nuova strategia di “ Prevenzione centrata
sulla persona” di malattie trasmissibili e non trasmissibili richiede l’adozione nella sanità pubblica del
paradigma della Medicina centrata sulla persona la cui definizione di salute è “ La scelta delle
migliori possibilità per essere la migliore persona umana”, che deve essere
formalizzata urgentemente dalla WHO
The continued
production of variants of SARS-COV 2 due to the change of the Spike Proteins
Receptor Binding Motif caused by the characteristics of the virus and the mass
vaccination in epidemic time that promotes the immune evasion of the virus,
leads to a delay in the production of vaccines after infections and clinical syndromes, which
cannot prevent the spread of new infections. In addition, mRNA vaccines are
genotoxic and cause a large incidence of even fatal adverse effects that have
led in some states to the suspension of any vaccination in children-adolescents
and young people under 39 years.
The
prevention of COVID-19 in Italy has been entrusted since December 2021 to a
mass vaccination with experimental vaccine sera mrna and adenovirus vectors
from monkeys and aborted fetuses whose DNA is hybridized with high probability
in the DNA of the vaccinated, increasing the likelihood of autoimmune diseases
and other even psycho-neurological problems.
Before 2021 and after there was no secondary prevention in the
population at risk, elderly people with comorbidities and people with
atherosclerotic pathologies, despite research on SARS-COV of 2002-2003, and
MERS 2009-2019, disappeared without vaccines with herd immunity. Primary
prevention was limited to lock-down, distance teaching, the use of facial masks
and hand washing (without indicating virocid temperature) and their
disinfection along with touched objects, Simple technologies known for years to
block virus transmission have been omitted.
An obsolete epistemological perspective and serious omissions in the
organization of prevention have led to the "lockdown", vaccine
obligations without scientific validation of the possibility of infection,
penalizing work and the economy. The use of masks and distance learning have
penalised the mental health of children and adolescents and prevented the
establishment of herd immunity by exposing children to increased vulnerability
to other pathogens. Errors and omissions in primary prevention and the omission
of secondary prevention in the population with comorbidities (93% of
mortality), caused in Italy more than one hundred thousand deaths and millions
of deaths worldwide. The wrong indications for early home care "
Tachypyrin and vigilant waiting" by
the Italian Health Minister and the rejection of effective hospital therapies
such as hyperimmune convalescent serums have caused thousands of deaths.
Currently the
speed of the continuous production of VOC (Variables of Concern) and the
ineffectiveness of previous vaccinations for the "Original antigenic sin
and immunodepression caused by multiple shots, always leads to a delay in the
production of vaccines mRNA effective, but evanescent and dangerous for the
induction of cell methylation of the whole body that increases vulnerability to
cancer. Pfizer’s clinical trial of mRNA vaccines was also found to be
unreliable, particularly in children. The adverse effects of the epigenetic
earthquake are frequent and even fatal
There is an
urgent need for a change in primary and secondary preventive strategy and a
home organization of early care based on person-centered medicine, a paradigm
shift in medical science, which if practiced, would stop the epidemic at its starting.
The new strategy in the communicable and non-communicable diseases’ prevention
requires the adoption in public health of the Person-centered Medicine paradigm
whose definition of health is " The choice of the best possibilities to be
the best human person" which must be formalized urgently by the WHO.
______________________________________________________________________________
Il problema della continua produzione di varianti dovuta alla
caratteristica del virus SARS-COV 2, cugino dello HIV, anche per l’attacco alle
difese immunitarie era stato previsto. Infatti nella prevenzione di secondo
grado del rischio di sindrome grave il rapporto CD4/CD8 anche nel COVID-19 è
uno degli indicatori. Le epidemie
SARS-COV 2 (2002-2003) e la pericolosissima MERS (2009-2010) sono scomparse in
un anno senza vaccinazione di massa, grazie all’immunità di gregge, incentivata
dai bambini e dagli adolescenti, con infezioni asintomatiche che hanno permesso
la circolazione del virus e l’immunità naturale e senza vaccinazione di massa.
Da tempo si sa infatti che la circolazione dei virus produce l’immunità. I
bambini oggi infatti sono maggiormente esposti a malattie trasmissibili grazie
all’errore della costrizione con le mascherine a scuola. Ogni settimana i
siamo contagiati da un virus nuovo e
metà del nostro DNA è di origine virale, ma l’immunità naturale li neutralizza.
Se si facesse un tampone per il meningococco metà della popolazione
risulterebbe attiva. Batteri e virus patogeni sono presenti nel nostro
organismo ma neutralizzati dall’immunità a memoria antigenica o per difese
naturali umorali. I beta-glucani dei saccaromiceti che formano immuno-complessi
con i virus e i batteri vaccinando
naturalmente [2]
probabilmente sono stati i nostri più potenti alleati nell’evoluzione per la
sopravvivenza della specie “uomo”.
L’inizio della pandemia è stato caratterizzato da un errore
epistemologico che ha determinato cinque milioni di morti a causa d’ignoranza
scientifica o malafede per ragioni di profitto. L’epidemia è stata infatti
affrontata con l’obsoleto e sbagliato
modello determinista,meccanicista imperante virus- rischio di malattia-
rischio di morte, contro l’ABC attuale dell’epistemologia medica : virus-
allostasi , resilienza/vulnerabilità, protezione/rischio- patogenesi clinica per l’insufficienza di
fattori protettivi, sindrome grave, rischio di morte.[3] [4]
La mancata adozione dell’attuale e corretto modello epistemologico della
salute, ispirato alla Medicina centrata sulla persona[5] [6]e
alla World Health Charter [7]
“La scelta delle
migliori possibilità per essere la migliore persona umana” [8] [9]
è stata determinante nel promuovere
un modello preventivo fallimentare. Libertà,verità,responsabilità, maturità
etica ed affettiva sono inseparabili dalle mondo delle variabili biologiche [10]
In Italia l’omissione della prevenzione
secondaria, (individuazione dei pazienti a rischio, prevenzione
secondaria, e organizzazione delle cure
domiciliari con farmaci e sostanze naturali efficaci), l’insistenza anche
difesa giuridicamente e vittoriosamente dal Ministro della sanità di una linea
guida (raccomandazione-ma non prescrizione) [11] per
una terapia precoce inefficace e pericolosa (“Tachipirina e vigile attesa”)[12],[13]
scelte legislative senza validazione scientifica che hanno spaccato il paese e
danneggiato migliaia di cittadini (“ il Green Pass”) , lo scarto di terapie
efficaci nelle COVID gravi come l’uso del siero iperiummune dei convalescenti,[14] [15]
l’induzione della vaccinazione in bambini e adolescenti senza rischio
epidemiologico di gravi COVID e che in altri paesi come la Svezia sono state
sospese, sono state la causa di più di centomila morti solo nella prima fase
dell’epidemia, evidenziando che la “pandemia degli asini”, e poco trasparenti
accordi del presidente dell’Unione Europea ad usum di BIG-PHARMA, sono stati
determinanti una strategia perdente a danno della popolazione. La vaccinazione
di massa contro un virus in tempo di
epidemia è noto ai non analfabeti che
induce mutazioni per evadere
l’immunità da parte del virus, fatto che si unisce alle caratteristiche del
virus stesso altamente mutante come lo HIV. La
cosa sorprendente ma spiegabile con la logica del profitto, è che
BIG-PHARMA dl 2007, quando è stato scoperto che la proteina N era comune a
tutti i Corona-virus,(ca 95%) non ha fatto vaccini contro questo antigene, che
presiede alla replicazione del SARS-COV 2 ,
mentre Maurizio Federico,
direttore del Centro per la salute globale dello ISS, ha ideato un pan-vaccino proprio contro la N
che il principe degli analfabeti (naturalmente in materia medica e
scientifica) che purtroppo ancora guida
la sanità italiana ha supportato e sta
supportando in modo ridicolo. L’immunità
contro la N è la causa della resistenza
alla grave infezione di metà della popolazione soprattutto dei bambini e
adolescenti già contagiati da corona-adenovirus, determinando una forte memoria
immunitaria, in caso d’infezione, a cui bambini e giovani sono meno vulnerabili
a causa della salute delle loro membrane cellulari, e che comunque esiste nel
50% della popolazione. Questo
costituisce un rischio per i soggetti giovani causato dai vaccini vettoriali in
quanto la forte reazione immunitaria contro il vettore può produrre immuno-complessi con reazioni trombofiliche
anche mortali,come si è verificato in adolescenti altrimenti sani che sono
morti. Inoltre essendo distrutto il vettore viene distrutto lo RBM (Receptor
Binding Motif) delle spike proteins
portato da questi e quindi
l’induzione immunitaria contro le “S-proteins”.
I bambini e i giovani, non a rischio epidemiologico, resistenti anche grazie all’integrità non
aterosclerotica delle membrane cellulari, senza “zattere lipidiche”-vedere la
teoria della relatività all’ingesso del virus nelle cellule-[16] e per la forte immunità umorale, due
condizioni poco presenti nell’anziano, il quale essendo immunosenescente non ha
una un’immunità cellulare acquisibile per un periodo di tempo garante di
serenità, e ha problemi per questo nell’induzione della memoria dei
linfociti T e B [17] ,
in quanto c’è una riduzione della sinapsi antigenica a causa della riduzione
dell’attivazione dell’espressione MHC1. E questo il motivo della strage causata
negli anziani con comorbidità nel 2020-2021.
La filosofia di
BIG-PHARMA e dei suoi mediatori in Europa e nei vari stati è stata:
“Se creo una domanda
messianica di vaccini mutanti il profitto aumenta perché gli stati mi chiedono
continuamente vaccini contro le mutazioni”
BIG-PHARMA e le lobby internazionali
intermediarie, di cui fa parte il
Ricciardi, docente dell’Università Cattolica , si sono arricchite . Tuttavia” il
diavolo fa le pentole ma non i coperchi”, infatti la produzione dei vaccini è
sempre in ritardo rispetto alle VOC (Variants Of Concern), che appaiono sul
“mercato” in continuazione.[18] Le
VOC sono sempre più rischiose perché la loro strategia è quella di evadere
l’immunità, mentre le poli-vaccinazioni deprimono l’immunità[19] e
se con lo stesso antigene ne annullano la possibile efficacia per soggetti non
immunosenescenti.
I vaccini mRNA sono
genotossici e pericolosi a causa dei cambiamenti delle basi nei mRNA nella loro
produzione . Infatti la sostituzione della pseudodouridina dello mRNA,fatta dai
produttori,con la N1-metilpseudouridina,produce un terremoto epigenetico, a
causa della metilazione indotta in tutte le cellule dell’organismo. Gli effetti
clinici di questo si rivelano negli effetti avversi gravi a breve, media lunga
scadenza, la cui incidenza non è ancora nota soprattutto sull’induzione dei
tumori. La tempesta di gruppi metilici
nelle cellule, metilante ance le altre basi, non è augurabile al peggior nemico
per questo motivo. Infatti i gruppi metilici si legano ai microRNA silenziando
la sintesi di proteine difensive e necessarie per la vita, come probabilmente
lo P53, gene oncosppressore. Inoltre lo mRNA vaccinale si lega ai geni
promotori certamente provocando dei silenziamenti dell’espressione genica. [20]
I sieri mRNA, diffusi
nel mondo sono stati sperimentati clinicamente in modo assolutamente
inattendibile e fallace se non truffaldino, come ha fatto rilevare Christine
Cotton, la più importante bio-statistica del mondo, come anche appare dal
campione insufficiente di 2400 bambini 5-12 reclutati per la sperimentazione
clinica, in cui gli effetti avversi sono stati seguiti solo fina a due mesi con
regole dell’AIFA per la registrazione delle segnalazioni spontanee di effetti avversi da vaccini solo entro 15
gg. Queste verità, non considerate anche dalla cupola sanitaria italiana, che
ha brillato per analfabetismo scientifico a danno della popolazione, sono stati
anche all’origine della morte del Nobel Luc Montagnier, a cui il fulgido
Bassetti, vero “scienziato da talk shows”, diede del “rincoglionito con demenza
senile”. La competenza scientifica di
Montagnier consigliava un’assoluta prudenza che l’ha portato a essere fiero
avversario della somministrazione di questi
vaccini, la cui metodologia
sperimentale è stata ridicolizzata e analiticamente confutata da Christine
Cotton, anche nella recente audizione al
senato francese [21].
Siamo di fronte alla malafede quando appare la singolare omissione nei rapporti
sulla sperimentazione clinica di gravi effetti avversi neirologico di cui una
vittima è stata ragazzina volontaria nella sperimentazione farlocca 5-12 della
Pfizer, Maddie De Garay, costretta alla sedia a rotelle.
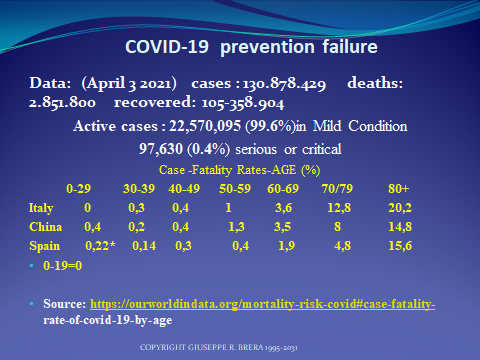
“In Italia tassi d’incidenza di decessi
attribuibili solo per il 50%, secondo un studio inglese, [22]
al COVID-19 dei bambini e
adolescenti è stato dall’inizio
dell’epidemia al febbraio 2022 da 0-9 anni di 3 casi su un milione , da 10-19,
4 casi su un milione, da 20-29 di 1 caso
su 100.000, da 30-39 di 5 casi su 100.000, 40-49 1 su 10.000, da 50-59 di 5 su
10.000. La rara mortalità per gli
adolescenti è associata alle comorbidità. [23] L’attribuzione diretta della mortalità al
COVId-19 per la fascia d’età 0-19,
evidenzia la riduzione ulteriore del
rischio epidemiologico, quasi assente. L’evidenza scientifica di gravi effetti
epigenetici per il silenziamento dei micro-RNA, e per l’inibizione
dell’immunità naturale[24] rende
assolutamente pericolosa la vaccinazione di bambini, adolescenti e giovani
la cui immunità naturale rende l’infezione rara e prevalentemente asintomatica. La probabilità del rischio di mortalità
per altre cause, rispetto a quella attribuita
al COVID-19, dai dati ISTAT è apparsa essere 171 volte superiore per la
fascia 0-9, di 52 volte per 10-19, di 34 volte per 20-29, di 18 volte 30-39, 11
volte per 40-49 di 14 volte per 50-59.
L’incidenza delle segnalazioni
di eventi avversi sulla popolazione 5-16 anni raccolti su segnalazioni
spontanee,oggetto di studio dell’AIFA , corrispondente a 1.941.680 persone
vaccinate nel primo mese di vaccinazioni
è stato di 1170 segnalazioni di cui 278
gravi, comprendente la mortalità. Queste segnalazioni spontanee sono molto
inferiori alla realtà. Solo su questi
dati, il tasso d’incidenza degli effetti avversi in questa popolazione,
altrimenti sana senza vaccini, appare
0.0006 ( 6 su 10.000) di cui 1 persona su 10.000 con effetti gravi
(0.0001), senza computare gli effetti avversi prevedibili a lungo termine, dovuti
all’alterazione epigenetica dei vaccini che prevedono una maggiore
vulnerabilità per tumori, malattie autoimmuni, disturbi dell’apprendimento e
del comportamento dovuti alle alterazioni
neurobiologiche. Il rischio di effetti avversi appare molto
grave e non è giustificato da una vaccinazione inutile per bambini, adolescenti
e giovani, non a rischio clinico. [25]
C’è un impressionante rischio
di miocardite negli adolescenti e nei
giovani, , altrimenti sani anche
documentato da numerose ricerche) e di altri effetti avversi gravi ( 1 su
10.000), e equivalenti ai ricoveri 12-19
( 1 su 10.000). ( fonte dei dati grezzi: dati AIFA). [26]
Come mai non è stata interrotta la vaccinazione dei bambini e degli adolescenti
già iniziata senza basi epidemiologiche ?
In
Svezia la vaccinazione negli adolescenti
12-17 non è più raccomandata ( aveva già sospeso lo mRNA
Moderna) in quanto i rischi sono
superiori ai benefici. La vaccinazione
per i bambini era già stata consigliata
solo per bambini fragili.
La
cosa soprendente in Italia è stata la politica preventiva nelle scuole affidata
a “banchi a rotelle” ( Azzolina –Ministro Istruzione II° Governo Conte), e alle mascherine (
Bianchi Ministro Istruzione governo Draghi) influenzata dalle omissioni dello
ISS, che era sorprendentemente all’oscuro dell’esistenza di semplici tecnologie
per l’emissioni id Ioni negativi con un quasi totale annullamento (99,99 %) dei
virus sospesi in aerosol,[27]
fatto che ha danneggiato lavoratori e studenti e anche parlamentari, con gravi
conseguenze a ogni livello.
Le uscite mediatiche di virostar televisive del coordinatore del
Comitato tecnico scientifico italiano, del presidente della Società Italiana di
Pediatria, del Direttore scientifico del Mario Negri, per indurre la vaccinazione
di bambini e adolescenti oggi sono
oggetto d’inchiesta della magistratura.
La cosa sorprendente
nella scellerata politica sanitaria dei governi Conte e Draghi, guidata dal
principe degli analfabeti, è stata l’assenza di una politica di prevenzione
secondaria sulla popolazione a rischio, prima della disponibilità dei sieri,
che ha causato più di centomila morti, fino al DL “ Untori” ( “Green Pass”) ,
senza alcuna base scientifica connotato dalla fulgida frase del totem
messianico Mario Draghi : “non
ti vaccini, contagi, muori, o fai contagiare e fai morire”. (22 Luglio 2021) che ha ulteriormente spaccato il
paese danneggiando moralmente e materialmente il personale sanitario e i
lavoratori, che si sono sottratti alla vaccinazione mRNA per cultura e
diffidente giusta prudenza. Vaccinati e
non vaccinati invece hanno la stessa probabilità di essere contagiati e
contagiare, ma non di morire. Tutto dipende dall’immunità naturale o indotta e
dalla qualità delle cure precoci. La pandemia degli asini è stato il vero
problema della sanità italiana, a danno della popolazione.
Il dr Giuseppe Remuzzi
del Mario Negri, ha affermato in intervista
:
… Che cosa direbbe ai genitori,
che hanno paura a vaccinare i propri bambini?
…Direi loro che non c’è nessun
motivo valido per non vaccinare i bambini. Questi sono i vaccini più efficaci e
più sicuri che siano mai stati prodotti per qualunque altra malattia. Sono più
sicuri non solo degli altri precedenti vaccini, ma anche di qualsiasi farmaco,
compresa l’aspirina….[28]
Nel merito della diffusione dell’epidemia il Remuzzi inoltre
dichiara:
“La seconda ragione è data dal fatto che abbiamo ancora fra i
cinque e i sei milioni di non vaccinati. Sono
loro che sostengono la diffusione del virus…..”[29]
Queste affermazioni senza
validazione scientifica si uniscono purtroppo a quelle ufficiali del Mario
Negri, considerate “Fake news” confutate da Christine Cotton,
“Fake News “I vaccini anti Covid-19 sono
stati approvati troppo velocemente e quindi non sono sicuri. I vaccini sono sicuri. Prima di essere autorizzati all’utilizzo
dalle autorità competenti devono superare tutte le prove di sicurezza ed
efficacia.”
E’ sorprendente che un illustre
ricercatore come Remuzzi, che con Feddy Suter ha annullato la politica del trattamento precoce del
Ministero della salute ,[30] con un errore abbia
adottato la “ strategia dell’untore”
per indurre alla vaccinazione, e sia all’oscuro delle ricerche sul terremoto
epigenetico prodotto dai vaccini mRNA inducente la depressione del sistema
immunitario e della importante ricerca (Science Translational Medicine) che
documenta che i vaccinati non sono
protetti da vaccini costruiti da varianti precedenti. [31]
Contrariamente alle asserzioni
del ricercatore non aggiornato e che si
permette di diffondere informazioni
senza validazione scientifica , la ricerca epidemiologica mostra in modo
inconfutabile un’associazione tra infezioni VOC ( Variants of Concern) e
vaccinazione e quindi il rischio di contagiare da parte dei vaccinati è almeno
equivalente rispetto ai non vaccinati, fatto che era già noto da tempo [32]
“…Logistic regression analysis showed that
full vaccination was significantly associated with infection by the Beta,
Gamma or Delta variants compared to the Alpha variant (adjusted OR: 3.1 (95%
CI: 1.3-7.3); 2.1 (95% CI: 1.1-4.2); 1.8 (95% CI: 1.4-2.4); respectively”
L’analisi
della regressione logistica (tecnica statistica che il peso delle associazioni
tra variabili” ha mostrato che una completa
vaccinazione è associata significativamente a infezioni da varianti Beta,
Gamma, Delta in confronto con la Alfa ( OR aggiustato : OR: 3.1 (95% CI:
1.3-7.3); 2.1 (95% CI: 1.1-4.2); 1.8 (95% CI: 1.4-2.4); rispettivamente [33]
Questo paradosso puo’ trovare
spiegazione nel fatto che la sequenza aminoacidica mutante dello RBM nelle spike proteins presente nei vaccini in
produzione e marketing arriva sempre
dopo l’epidemia da variante , [34] e se ripetutamente inoculata porta al peccato
antigenico originale e alla immunodepressione causata da ripetuti dosi di
vaccini mRNA.[35] [36] [37]
Purtroppo l’ignoranza epistemologica e scientifica della
cupola sanitaria non solo italiana,mondiale , europea (comprendendo gli
“oversea” tipo Antony Fauci) basata sull’ obsoleto modello determinista e
meccanicista monofattoriale dell’idea della salute,[38] sponsorizzato in Europa dal suo presidente e
dal commissario europeo alla sanità, è
stato determinante per milioni di morti, facendo verificare il fallimento di
questa impostazione che struttura l’attività resiliente del sistema immunitario
solo su un’immunità acquisibile artificialmente non prima alla protezione
immunitaria naturale facilmente rinforzabile con un’adeguata dieta e banali
nutraceutici.
Avevamo comunque comunicato il rischio epigenetico dei mRNA
all’EMA e all’AIFA prima dell’autorizzazione vaccinale ai bambini e questi dovranno vedersela con la magistratura
insieme a Speranza anche per il suo paradigma preventivo che ha portato a
un’omissione dell’organizzazione di efficaci cure domiciliari. In un mese di
vaccinazione l’incidenza degli affetti avversi gravi nei 5-12 è stata 1/10.000. In questa fascia d’età
il rischio
Sulle VOC è comparso un articolo importante su Science [39]
che discute la rapida selezione della varianti che progressivamente aumentano
la loro evasione dall’immunità vaccinale
della popolazione.
“The strains that look poised to drive the latest
comeback are all subvariants of Omicron, which swept the globe over the past
year. Several derived from BA.2, a strain that succeeded the initial BA.1
strain of Omicron but then was itself outcompeted in most places by BA.5, which
has dominated in recent months. One of these, BA.2.75.2, seems to be spreading
quickly in India, Singapore, and parts of Europe. Other new immune-evading
strains have evolved from BA.5, including BQ.1.1, which has been spotted in multiple
countries around the globe.”
Le figlie
della variante B5, come la BA.2.75.2
sono ormai circolanti e gli anticorpi monoclonali disponibili non sono
attivi.
L’evidenza
che la popolazione non possa essere sottomessa a poli-inoculazioni di richiami
di vaccini che hanno un’alta frequenza di effetti avversi, possono indurre
gravissime conseguenze sulla salute a
medio e lungo termine. Questo comporta l’urgente necessità di una cambio di paradigma e di strategia nella sanità pubblica , fatto da persone comptenti
non da politici praticanti analfabeti o semianalfabeti in materia di “Prevenzione
centrata sulla persona” con una nuova
organizzazione tettitoriale ed istituzionale,
puntando su misure di educazione in accordo con il cambiamento di
paradigma della medicina.[40]
Questa nuova
politica sanitaria deve prevedere:
a. Il passaggio generale del sistema
sanitario italiano alla Medicina centrata sulla persona, cambiamento di
paradigma della Medicina che centra il sistema sulla educazione alla salute,la
prevenzione , la “self care”e la formazione dei medici al metodo clinico
centrato sulla persona. [41] [42]
[43]
Il cambiamento di paradigma permette un aumento delle risorse soggettive
, con un grande beneficio anche per l’economia e il lavoro e un enorme
risparmio di spese sanitarie[44]
b. Abolizione del DL “Green pass” e
reintegro immediato persone sospese perché non vaccinate
c. Educazione alla salute a una corretta
qualità della vita e a una dieta antivirale arricchita da nutraceutici con una
potente documentata ed efficace azione preventiva delle malattie trasmissibili
e delle gravità cliniche [45]
[46]
d. Introduzione nelle scuole e negli
ambienti di lavoro chiusi di macchine
per l’emissione di ioni negativi che annullano i virus nell’aerosol, e riducono
la vulnerabilità all’infezione anche grazie all’indotta modifica
elettromagnetica delle membrane cellulari e l’alcalinizzaione plasmatica [47]
e. Individuazione pazienti a rischio di
COVID-19 grave (anziani con comorbidità) e “prevenzione centrata sulla persona”
con l’allostasi antivirale e l’immunostimolazione preventiva [48]
f. Esclusione dei pazienti oncologici
dalle vaccinazioni mRNA dalla lista dei pazienti “fragili”, alla luce dell’evidenza epidemiologica di un
aumento d’infezioni , ricoveri e mortalità in vaccinati. [49]
Attualmente il Ministero della salute raccomanda vaccinazione e richiami ai
pazienti oncologici o in remissione.
g. Organizzazione cure domiciliari con farmaci e
antivirali efficaci
h. Introduzione nelle cure ospedaliere dei
sieri iperimmuni di convalescenti per i
pazienti gravi.
Una
prevenzione primaria e secondaria “Centrata sulla persona” e una terapia precoce bene organizzate sono
sicuramente più efficaci e non pericolose, rispetto agli attuali sieri
vaccinali, per neutralizzare il rischio delle varianti e di altre malattie trasmissibili con un effetto indiretto anche nella prevenzione
di malattie non trasmissibili come il cancro e le malattie cardio-vascolari.
Questo
cambiamento di prospettiva è possibile solo se il sistema sanitario italiano si
orienta alla Medicina centrata sulla persona, cambiamento di paradigma della
medicina.[50]
[1] Presidente del Comitato Sanitario Nazionale e
dello World Health Committee. Direttore della Scuola Medica di Milano,
presidente della Società Italiana di Adolescentologia e Medicina dell’Adolescenza
[2]
Brera G.R. A
Columbus's egg: the possibility of beta-glucan-induced TRIM and adaptive
immunity against COVID-19, inducing cross primary and secondary prevention for
the pandemic shutdown worldwide. Scientific
Reports of the Milan School of Medicine. 2022; 2 DOI
[3] Brera G.R. Rischio zero per il COVID-19
con la dieta anti virale.: Manuale di allostasi anti-virale e immunostimolazione preventiva. Milano,
Università Ambrosiana ed; 2022
[4] Brera, G.R. Person-Centered Medicine and Person Centered Clinical Method.
Milano: Università Ambrosiana ed.: 2021
ISBN: 9798726465432 (II°
edizione)
Distribuzione
Mondiale Amazon
[5] Brera G.R. Person-centered
Medicine: Theory, Teaching, Research. Int.J.Pers. Cent.Med 2011; 1
(1):69-79
[6] Brera G.R. . Person-centered Medicine and Medical
Education in third Millennium (with the introduction of Iosef Seifert The
seven aims of Medicine it.) Roma- Pisa: IEPI ;2001 (Italian)
[7] The World Health Charter Proceedings of the International Conference: Medical Science and Health Paradigm
Change 13-14-15 October 2017 Milano, Regione Lombardia, Italia, Ospedale
Maggiore – Ca Granda
[8] WHO
Person-centered Medicine and Medical Education. (internet)
Geneva:WHO Symposium; 4 May 2011. Internet:
http://www.unambro.it/html/pdf/All_Symposium_Education_People_Centred_4May2011.pdf
[9]
Ibidem 3
[10] Brera, G.R. Person-Centered
Medicine and Person Centered Clinical Method. Milano: Università Ambrosiana ed.: 2021 ISBN: 9798726465432 (II° edizione)
Distribuzione
Mondiale Amazon
[11] Sentenza Consiglio di Stato sez III° n° 207
19 Gennaio 2022 su Sentenza TAR Lazio SEz. III° n° 419 del 15 Gennaio 2022
Internet https://www.sanita24.ilsole24ore.com/art/sentenze/2022-01-17/la-circolare-vigile-attesa-ministero-sa...
[12]
Pandolfi S, Simonetti
V, Ricevuti G, Chirumbolo S. Paracetamol in the home treatment of early
COVID-19 symptoms: A possible foe rather than a friend for elderly patients? J
Med Virol. 2021 Oct;93(10):5704-5706. doi: 10.1002/jmv.27158. Epub 2021 Jun 30.
Erratum in: J Med Virol. 2022 Mar;94(3):1246. PMID: 34170556; PMCID:
PMC8426871.
[13] L’AIFA indica ancora ora la Tachipirina
come primo farmaco per le cure domiciliari contro le evidenze scientifiche
.
[14] Perotti C, Baldanti F, Bruno R, Del Fante
C, er al., Covid-Plasma Task Force. Mortality reduction in 46 severe Covid-19
patients treated with hyperimmune plasma. A proof of concept single arm
multicenter trial. Haematologica. 2020 Dec 1;105(12):2834-2840. doi:
10.3324/haematol.2020.261784. PMID: 33256382; PMCID: PMC7716363
[15]
Yuwono Soeroto A,
Purwiga A, Alam A, Prasetya D. Plasma convalescent decrease mortality in
COVID-19 patients: a systematic review and meta-analysis. Eur Rev Med Pharmacol
Sci. 2021 Jul;25(14):4841-4853. doi: 10.26355/eurrev_202107_26398. PMID:
34337734.
[16] Brera G.R. SARS-COV 2
allostasis and the people and person-centered prevention. A new prevention
strategy based on a people metabolic and immune shield for the pandemic
shutdown.
Part
1 The Sars-Cov 2 entry and COVID-19. Milan. Università Ambrosiana , 2021.
ISBN: 9798530093906 Distribuzione Mondiale Amazon
[17]
Vogel G. New Omicron
strains may portend big COVID-19 waves. Science. 2022 Sep 30;377(6614):1479.
doi: 10.1126/science.adf0777. Epub 2022 Sep 29. PMID: 36173845
[18] Brera G.R . SARS-COV 2-
allostasis and the people and person-centered prevention.
Part 2 The Sars-Cov 2- induced immunosuppression nd covid-19 anergy .
Part 3 The antiviral metabolic allostasis and
preventive immunostimulation -How to
induce zero risk for covid-19.
Milan: Ambrosiana University:
ISBN: 9798547583520
Distribuzione
Mondiale Amazon
[19] Seneff, S., Nigh, G., Kyriakopoulos,
A. M., & McCullough, P. A. (2022). Innate immune suppression by SARS-CoV-2
mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food
and chemical toxicology : an international journal published for the British
Industrial Biological Research Association, 164, 113008. https://doi.org/10.1016/j.fct.2022.113008
[20]
Lockhart J, Canfield J, Mong EF, Vanwye J, Totary-Jain H. Nucleotide
Modification Alters MicroRNA-Dependent
Silencing of MicroRNA Switches. Mol Ther Nucleic Acids. 2019;14:339-350.
doi:10.1016/j.omtn.2018.12.00
[21]
Christine Cotton
Udizione presso il Senato Francese del 22 Aprile 2022: Evaluation des pratiques
méthodologiques mises en œuvre dans les essais Pfizer dans le développement de
son vaccin ARN-messager contre la COVID-19 en regard des Bonnes Pratiques
Cliniques Présentation OPECTS Christine COTTON 1 A Maxime Beltra Christine
COTTON – 05/04/2022 - © L
Internet : https://christine-cotton.1ere-page.fr/audition-opecst-christine-cotton/
[23] McCormick
DW, Richardson LC, Young PR, et al.Pediatric Mortality Investigation Team.
Deaths in Children and Adolescents Associated With COVID-19 and MIS-C in the
United States. Pediatrics. 2021 Nov;148(5):e2021052273. doi:
10.1542/peds.2021-052273. Epub 2021 Aug 12. PMID: 34385349.
[24]
Ibidem 17
[25] Brera G.R. Scientific evidence of mRNA and vectorial
vaccines genotoxicity inducing tumors and psycho-neuro-behavioral disorders.
https://www.researchgate.net/publication/356588024 I
DOI: 10.13140/RG.2.2.29151.18081
[26] AIFA 11 rapporto di sorveglianza Vaccini
COVID-19
[27] Brera G.R Rischio zero per il COVID-19
con la dieta anti virale.: Manuale di alllostasi anti-virale e
immunostimolazione preventiva. Milano, Università Ambrosiana ed.; 2022 Distribuzione mondiale Amazon
[28]
Intervista da Sparaynews https://www.spraynews.it/post/giuseppe-remuzzi-direttore-istituto-mario-negri-aprite-le-
scuole-ma-vaccinate-i-bambini 5 G ennaio
2022
[29] Giuseppe Remuzzi Ibidem 25
[30] Suter F, Consolaro E, Pedroni S, Moroni C,
Pastò E, Paganini MV, Pravettoni G, Cantarelli U, Rubis N, Perico N, Perna A,
Peracchi T, Ruggenenti P, Remuzzi G. A simple, home-therapy algorithm to prevent
hospitalisation for COVID-19 patients: A retrospective observational
matched-cohort study. EClinicalMedicine. 2021 Jul;37:100941. doi:
10.1016/j.eclinm.2021.100941. Epub 2021 Jun 9. PMID: 34127959; PMCID:
PMC8189543. (Medrix 25/03/2021)
[31] Andeweg SP, Vennema H, Veldhuijzen I,
Smorenburg N, Schmitz D, Zwagemaker F, van Gageldonk-Lafeber AB, Hahné SJM,
Reusken C, Knol MJ, Eggink D; SeqNeth Molecular surveillance group†; RIVM
COVID-19 Molecular epidemiology group†. Elevated risk of infection with SARS-CoV-2 Beta,
Gamma, and Delta variant compared to Alpha variant in vaccinated individuals.
Sci Transl Med. 2022 Jul 21:eabn4338. doi: 10.1126/scitranslmed.abn4338. Epub
ahead of print. PMID: 35862508.
[32] Federico M. The conundrum of
current anti-SARS-CoV-2 vaccines. 2021; Cytokine & Growth Factor Reviews. 60:46-51
[33] Ibidem 27
[34] Ibidem 27
[35] Federico M. Biological and immune responses to current
anti‐SARS‐ CoV‐2 mRNA
vaccines beyond anti‐Spike antibody production . Proceedings
of the Conference Person-Centered Medicine, prevention and adolescence;
III° Session: Person-centered prevention risks from
genetic vaccines ,early therapy of COVID-19; 2021 Nov.20 ; Milan, University
Ambrosiana. 2021.p 44-45.
[36] Seneff, S., Nigh, G., Kyriakopoulos,
A. M., & McCullough, P. A. (2022). Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of
G-quadruplexes, exosomes, and MicroRNAs. Food and chemical toxicology : an
international journal published for the British Industrial Biological Research
Association, 164, 113008. https://doi.org/10.1016/j.fct.2022.113008
[37]
Lockhart J, Canfield J, Mong EF, Vanwye J, Totary-Jain H. Nucleotide
Modification Alters
MicroRNA-Dependent Silencing
of MicroRNA Switches. Mol Ther Nucleic Acids. 2019;14:339-350. doi:10.1016/j.omtn.2018.12.00
[38] Brera,G.R. Person-Centered
Medicine and Person Centered Clinical Method.
Milano:UniversitàAmbrosiana
ed.: 2021 ISBN: 9798726465432 (II° edizione)
Distribuzione
Mondiale Amazon
[39] Vogel G. New Omicron strains may portend big
COVID-19 waves. Science. 2022 Sep
30;377(6614):1479. doi: 10.1126/science.adf0777. Epub 2022 Sep 29. PMID:
36173845.
[40] Università Ambrosiana. “ Medical Science and health Paradigm Change” G.R.
Brera ed.. Proceedings of the Conference Milan 13-14-15 October 2017. Milan; Università Ambrosiana: 2018 Intternet
www.health paradigm change.it
[41] Brera G.R
.Person-centered Medicine: Theory,Teaching,Research. Int.J.Pers. Cent.Med 2011; 1
(1):69-79
[42] Brera G.R.,
Violato C. Biava PM et al. Medical Science and Health Paradigm change. Milan, Ambrosiana University ed. ; 2017. Internet
https://www.researchgate.net/publication/324172109_Medical_Science_and_Health_Paradigm_change
[43] Brera G.R. Person-centered
Medicine and Medical Education in third Millennium (with the introduction vof Iosef Seifert The
seven aims of Medicine it.) Roma- Pisa: IEPI ;2001 (Italian)
[44] Brera G.R & ITFOP Person Centered Clinical Method
and its Teaching Results in Medical Practice.Paper presented in the Conference
“1 st International Symposium on new perspectives I medical education Assisi,
Italy, October 24, 2003” DOI 10.13140/RG.2.1.3374.5447 Internet
http://www.unambro.it/html/pdf/Person_Centred_Clinical_Method_Teaching.pdf
[45] Brera G.R . SARS-COV 2-
allostasis and the people and person-centered prevention.
Part 2 The Sars-Cov 2- induced immunosuppression nd covid-19 anergy .
Part
3 The antiviral metabolic allostasis and preventive immunostimulation -How to induce zero risk for covid- 19. Milan:
Ambrosiana University:
ISBN:
9798547583520 Distribuzione Mondiale Amazon
[46] Brera G.R Rischio zero per il COVID-19
con la dieta anti virale.: Manuale di alllostasi anti-virale e
immunostimolazione preventiva. Milano, Università Ambrosiana ed.; 2022 Distribuzione mondiale Amazon
[47] Ibidem
40
[48] Ibidem
39
[49] Wang W, Kaelber
DC, Xu R, Berger NA. Breakthrough SARS-CoV-2 Infections, Hospitalizations, and Mortality in
Vaccinated Patients With Cancer in the US Between December 2020 and November
2021. JAMA Oncol. 2022 Apr 8. doi: 10.1001/jamaoncol.2022.1096. Epub ahead of
print. PMID: 35394485.
[50] Ibidem 36